
We are currently working to update the Member Portal and the Board recently approved for the work to commence. These updates will include the feedback received from members as part of this process. We are hoping the current list of updates will be fully functioning early next year.
MSAC – New Item Numbers
MSAC – The Medical Services Advisory Committee are the body responsible for adding items to the MBS.
1. MSAC application 1632 PSMA PET/CT
We welcome the favourable recommendations from MSAC for public funding of PSMA PET/CT imaging contained in the newly released Public Summary Document. If accepted by Minister Hunt, MSAC’s positive recommendations represent an exceptional outcome for Australian men battling prostate cancer.
AANMS worked on this application for two years with Cyclotek, with the majority of funding coming from Astra Zeneca. We are currently working on a joint media release in readiness for the Minister’s announcement and will of course also complete our own media campaign to complement the above.
It is crucial that our announcements do not get in the way of the Minister’s, so we are waiting in anticipation to promote our association and the great work of nuclear medicine in general. We hope to work with prostate cancer support groups to advocate for the prompt implementation of this recommendation.
Key things to note are that the recommended wording of the item is tracer agnostic – allowing us to choose whichever PSMA agent we prefer.
2. MSAC application 1686 LuPSMA i&t
Lu PSMA i&t is currently being offered around Australia under the SAS and is approved by DVA for veterans for the treatment of end stage prostate cancer. There is no available funding, leading to inequitable access to treatment in this effective class of drugs for men suffering from a painful lethal condition.
We have accepted a request to co-sponsor this current application, which will mean a reasonable amount of work between now and mid February to meet the timelines for consideration by MSAC’s evaluation subcommittee (ESC) in June 2022. We have engaged the services of the HTA who was instrumental in our successful PSMA PET/CT application.
3. Other Diagnostic Imaging MSAC applications currently in the system – in brief
1562 – Streamlining MBS times for PET Project. Commissioned by MSAC to develop a new process for assessing the clinical utility of PET for FDG for avid rare cancers after lobbying by AANMS, and being raised in the recent MBS review.
The assessment tool developed is a generic economic model that has undergone a validation process and will be reviewed by the Evaluation Sub-Committee (ESC) at its June 2022 meeting.
The ultimate goal is to obtain a single FDG item applicable to ALL FDG avid tumours.
1643 – Amyloid PET and cerebrospinal fluid testing for Alzheimer disease. This is a co-application sponsored by Biogen as part of their attempt to get aducanumab listed on the Pharmaceutical Benefits Schedule (PBS). It is anticipated that this application will be considered at ESC at its June 2022 meeting. We have provided supportive letters.
Follow this link further details on any of these applications MSAC – Medical Services Advisory Committee
The Board also has a list of priority MSAC applications as advised by you via the membership survey of which we are currently reviewing and prioritising for next year.
The Association is regularly asked to contribute to consultation surveys as part of the MSAC process and we have a small group of members we call on regularly.
If you are interested in a particular subject matter or happy to have your name on a list of ‘go to’ members to assist in supporting/ assessing these applications, we would be very grateful. Please email aanms@aanms.org.au
Member Survey Results
We would like to thank everyone who took the time to contribute to the survey. There were six questions asked, five of those with multiple selection answers and the last question required free form comment. Here are the results in brief:
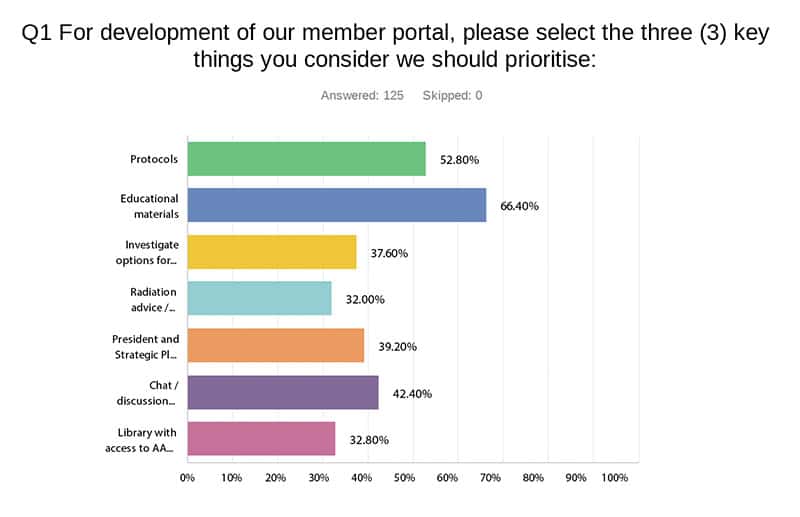
Educational Materials and Protocols scored quite highly for updates to the Member Portal.
We will be seeking further input and/or materials and information from members to contribute to the resources.
Q1 Answer choices & responses
- Protocols – 52.80% (66)
- Educational materials – 66.40% (83)
- Investigate options for development of CPD – 37.60% (47)
- Radiation advice / information – 32.00% (40)
- President and Strategic Plan Updates – 39.20% (49)
- Chat / discussion forums so that members can engage in policy discussions, ask for assistance, query protocols etc. – 42.40% (53)
- Library with access to AANMS submissions and/or other public documents – 32.80% (41)
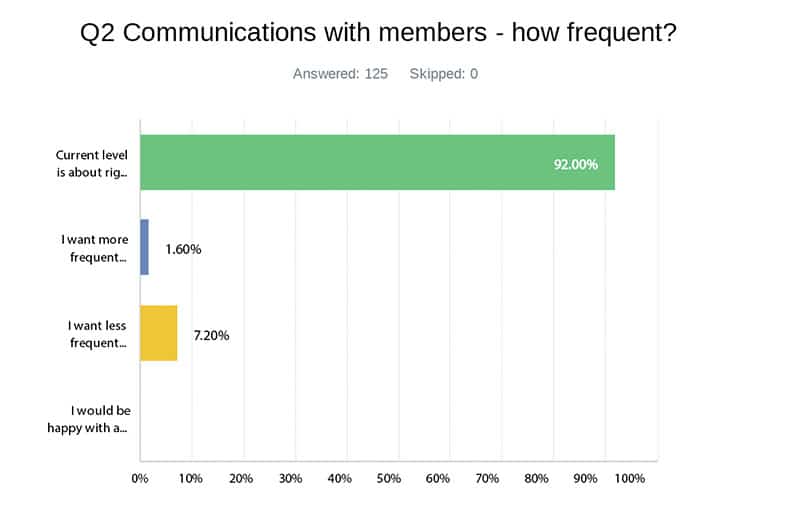
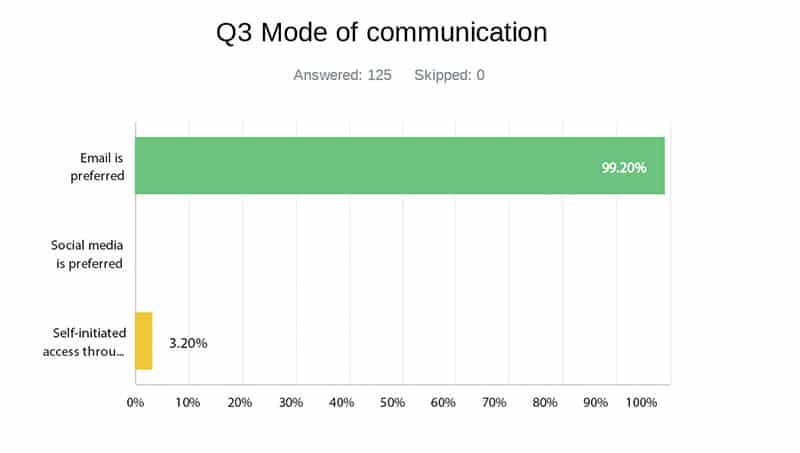
Overwhelming results on question 2 and 3, requiring no explanation.
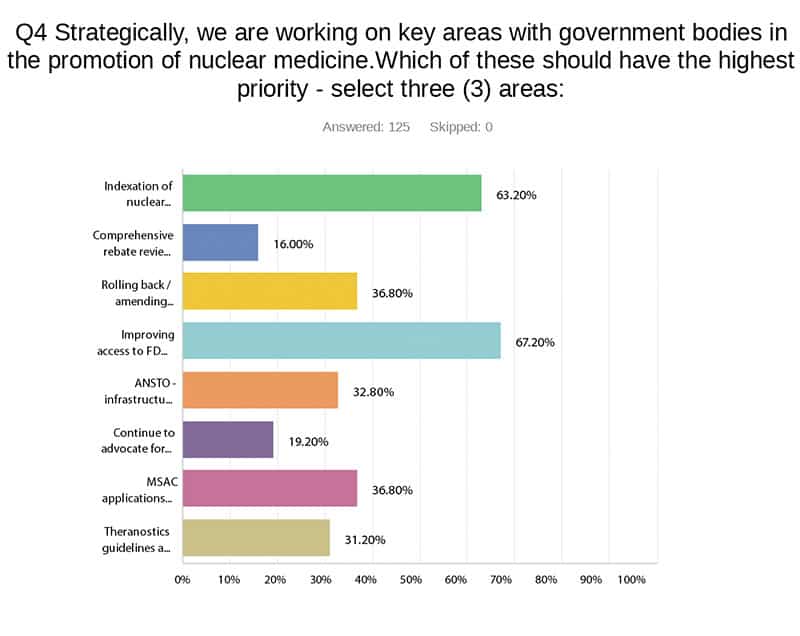
The two main areas were Indexation of rebates and improving access to FDG. As you can see, we are already working on the FDG issue with MSAC. In regard to Indexation, please see the detailed information on our strategy in this report.
Of the remainder, we will progress them as best we can considering resources and your given priorities. It is worth noting that we are currently working on all eight areas as follows:
- Rolling back amending cardiac MBS changes – one of our Board members is very active in this space and this is part of our strategic MSAC program for the new year. We have not given up though we think many have come to terms with the new equilibrium.
However the whole concept of the MBS telling referrers how to practice medicine is an important issue that we should not let slide as it may set an unfortunate precedent to the way the MBS is managed. - ANSTO infrastructure – the recent announcement re infrastructure spending was welcome news, as was the completion of the Building 23 seven-week maintenance program.
- We did take the opportunity, given the ANSTO announcement to contact Ministers, Shadow Ministers and other Health representatives and re-issue our indexation report.
- Continue to advocate for personal supervision – we have been in several meetings of late on this issue and the Department of Health is seeking our direct input into the discussion.
Q4 Answer choices & responses
- Indexation of nuclear medicine rebates – 63.20% (79)
- Comprehensive rebate review for highest volume items, e.g. bone scans – 16.00% (20)
- Rolling back / amending cardiac MBS changes – 36.80% (46)
- Improving access to FDG PET for all patients with cancer – 67.20% (84)
- ANSTO – infrastructure and supply issues – 32.80% (41)
- MSAC applications for new items – 36.80% (46)
- Theranostics guidelines and funding – 31.20% (39)
Of the list we are strategically planning to take on, in order of priority:
▪ Generic FDG PET for infection/inflammation
▪ Cardiac imaging (both SPECT and PET)
▪ Amyloid PET for Alzheimer’s
We continue to seek external funding for all MSAC applications as well as consider the option of applying for public funding through the MSAC application process.
Public funding through MSAC of course means handing over control of the process to MSAC but each application will be reviewed to select the best and most cost effective path.
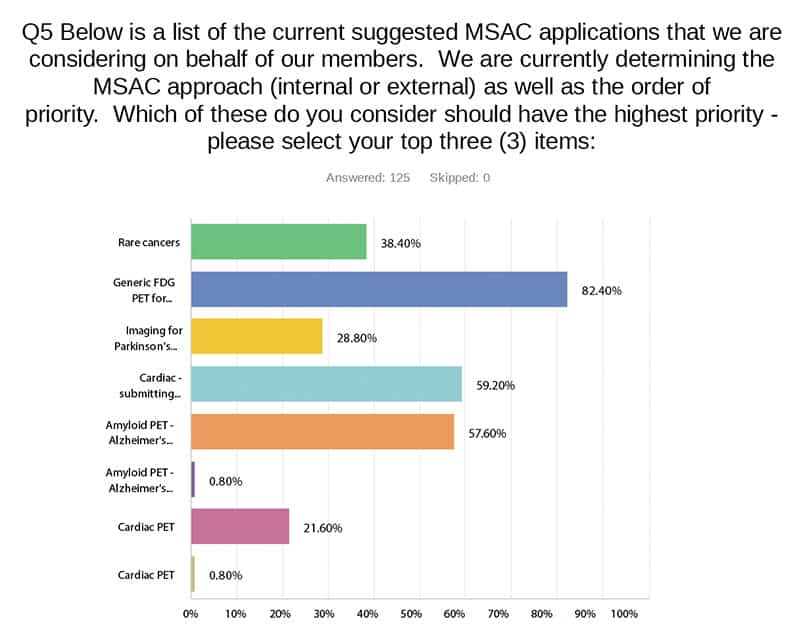
Q5 Answer choices & responses
- Rare cancers – 38.40% (48)
- Generic FDG PET for infection/inflammation item – 82.40% (103)
- Imaging for Parkinson’s disease – 28.80% (36)
- Cardiac – submitting evidence to remove current restrictionsAt the MBS Review discussions, one option we were given was to resubmit cardiac imaging to MSAC to have its current utility and efficacy re-evaluated – 59.20% (74)
- Amyloid PET – Alzheimer’s disease – 57.60% (72)
- Amyloid PET – Alzheimer’s disease – 0.80% (1)
- Cardiac PET – 21.60% (27)
- Cardiac PET – 0.80% (1)
Q6 – in this question we asked for your top three key issues not included in the Strategic Plan rolled out in May.
Four issues were raised almost equally within the response:
▪ Nuclear medicine education and resources
▪ MBS/MSAC and related
▪ Promotion of NM in general
▪ Theranostics
As this was a relatively broad question, our next survey will explore these further. In general, however all these items are currently on our list of priorities and we are encouraged by the feedback received.
Thank you again to all responders.
Federal Election Campaign – Indexation
A sub-committee of the Board have completed a selection process over the past two months to contract a campaign manager in a strategic push to get indexation of NM over the line.
We a very happy to report that we have started this work with CMAX Advisory and have a comprehensive and planned approached between now and the election. We shall keep our membership updated.
Brain FDG/PET Tutorials Online
Reminder to have a look at Chris Rowe’s excellent tutorials on how to read FDG PET for Dementia which can be accessed through the Australian Dementia Network (ADNet), of which Chris is the Director: Reading FDG PET scan tutorials
DIAC and Other Committees
Iain Duncan has officially taken over as the AANMS Representative on DIAC from Hugh Dixson who represented the Association in excess of 10 years.
The Board would like to thank Hugh for his time and the hours of work required throughout the years. Hugh has been a tireless servant of Nuclear Medicine over many years and I am sure welcomes some down time.
As part of our continuous improvement program as an Association we are currently formalising AANMS representation on committees. This formalisation will include ensuring the Board meets is obligation of care and diligence under the Corporations Act.
For those of you who are currently AANMS Representatives on external committees, our General Manager will be in contact to discuss.
Should any of our members want to become more involved in the Association, committee membership may be worth considering.
Please contact Lisa at gm@aanms.org.au if you would like to discuss this or any other potential role within the organisation.
RACP and Nuclear Medicine
As advised in my last update we recently supported an initiative to have rotation for basic physician trainees in Nuclear Medicine accepted as core training. This would encourage more physician trainees to test the water and hopefully improve physician interest in our specialty.
To further this conversation we are meeting with the RACP, including the incoming president, in early December to put our case more strongly and hopefully obtain assurances of their support and commitment to Nuclear Medicine.